
Jump to this Section
Understanding Gynecomastia Surgery in South Florida
Gynecomastia refers to the enlargement of male breast tissue, and it can affect men of all ages. The condition may be caused by hormones, genetics, weight fluctuations, or even certain medications.
And for many men, gynecomastia dips your levels of confidence, dials up your self-consciousness, and affects nearly every part of life, from the gym to dating to what clothes you wear.
Gynecomastia vs. Fat: Know The Difference
It’s important to understand the difference between gynecomastia vs. fat. While excess fat can cause a similar appearance, true gynecomastia involves glandular tissue that does not respond to diet or exercise alone. For gynecomastia men, this distinction matters when considering treatment options, especially surgery.
A Lasting Solution
Gynecomastia surgery, also called male breast reduction, is the most effective and lasting solution to men struggling with their body image. Dr. Elliot Jacobs offers advanced gynecomastia surgery in Boca Raton using minimally invasive techniques and personalized treatment plans. He’s treated over 5,000 cases across 30 years in practice, building up his reputation as a gynecomastia surgery national authority.

Types Of Gynecomastia in Men
Let’s face it: It really doesn’t technically matter the severity of your gynecomastia case, especially for overweight men or guys who’ve struggled with their body image for years. What’s really important is how you feel about your body. If your chest, small or large, holds you back, male breast reduction and Florida gynecomastia surgery with Dr. Jacobs may be right for you.
Mild to moderate gynecomastia may be frustrating, but severe gynecomastia can significantly distort the chest and create deep emotional discomfort. At Dr. Jacobs’ Boca Raton practice, we treat all levels of gynecomastia, from subtle to extreme, helping patients finally feel comfortable in their own skin.
Given the natural range of body types, shapes, and individual fat storage, excess male breast tissue can appear in many forms:
Slightly Enlarged, With a “Feminine” Look
Mild cases of gynecomastia give the chest a softer, rounded appearance. It may look subtle under certain clothes, but still impacts confidence.
Large, Pendulous, Fatty Breasts
These appear similar to female breasts and may include skin stretching. Surgery typically involves gland removal, liposuction, and skin tightening to reshape the chest’s overall volume and composition.
Puffy Nipples (on an Otherwise Trim Body)
Puffy, protruding nipples are most often caused by enlarged glands sitting just beneath the areola. This type is highly correctable with targeted gland removal.
Misshapen, Tuberous Breasts and/or Asymmetry
Tuberous breasts in men, often mistaken for puffy nipples or moderate gynecomastia, are caused by a constriction at the base of the breast, forcing tissue to grow outward and downward. This can result in puffiness around the nipples, asymmetry, or more pronounced deformities. Treatment typically involves gland removal and liposuction to address the puffiness, with skin tightening techniques for more severe cases. In rare situations, a mastectomy-like procedure can be undergone for truly corrective results.
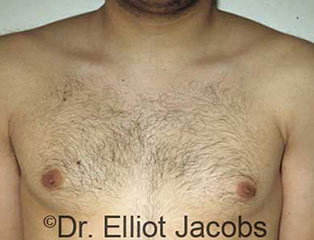
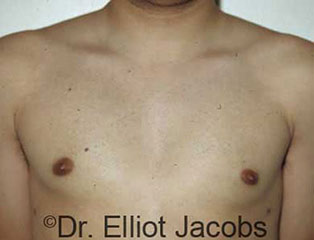
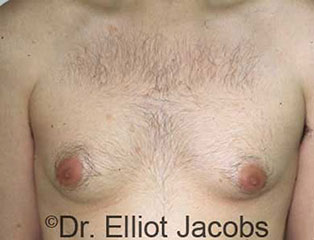
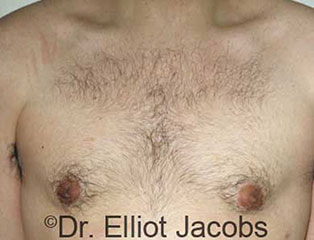
See Real Results from Boca Raton Gynecomastia Surgery
Want to see what’s possible with Dr. Jacobs? Browse before-and-after photos to view real results from actual patients.
Types of Gynecomastia Surgery in South Florida
Every guy is different, and so is his ideal vision for his appearance. This is exactly why Dr. Elliot Jacobs uses a wide range of science-backed gynecomastia techniques to customize treatment for his patients, many of which he pioneered himself across 30+ years of practice.
Whether you’re a teenager, a bodybuilder, or dealing with chest revision surgery, you’ll get expert care at Dr. Elliot’s premier Boca Raton practice serving nearly a dozen gynecomastia case types.
Traditional Gynecomastia
- Gland excision with or without liposuction.
- Small incisions at the areola or under the armpit
- Twilight sedation for comfort and quick recovery.
- Minimal scarring with natural-looking chest contour.
- Return to light activities within 3-7 days.
Adolescent Gynecomastia
- Performed responsibly once key growth stabilizes (usually post-puberty).
- Conservative approach to preserve future development or changes.
- Often involves small gland excision only.
- Fast recovery, ideal for high school-aged patients.
- Boosts self-esteem during formative years.
Crater Deformity Repair
- A unique correction of post-surgical chest depressions.
- Tissue grafts or fat transfer to rebuild contour.
- May include liposuction for symmetry.
- Custom treatment plan for each patient.
- Considered an outpatient surgery with minimal downtime.
Gynecomastia in Bodybuilders
- Precise removal of dense glandular tissue.
- Preserves muscle definition and symmetry.
- Typically no skin removal needed.
- Often no visible scarring when healed.
- Enhances chest aesthetics for competition-level results and a more representative self-image.
Gynecomastia for Overweight Men
- Often staged surgery with re-evaluation after 6-8 months.
- May involve gland excision and liposuction, as needed.
- Skin removal possible for severely stretched tissue.
- Mastectomy-style approach in severe gynecomastia cases.
- Goals customized for each man: a flatter or sculpted chest.
Revision Gynecomastia
- Fixes unsatisfactory results from previous surgery, cosmetic or not.
- Removal of residual gland or scar tissue.
- Addresses asymmetry or contour irregularities
- May involve fat grafting for better overall balance.
- Careful analysis and planning with Dr. Jacobs to minimize scarring and side effects.
Puffy Nipples
- Direct gland excision under areola.
- Leaves minimal or no-visibility scars thanks to advanced incision techniques.
- Twilight sedation and quick recovery.
- Restores a flat, natural-looking nipple area.
- High satisfaction rate for this common aesthetic concern.
Chest Asymmetry
- Customized gland and fat removal.
- May include fat grafting or skin tightening.
- Aims for size, width, and shape harmony between both sides of the chest.
- Often correctable in a single procedure.
- Tailored to your body for true, natural-looking chest harmony.
Scar Tissue Formation
- Often occurs from prior chest surgery or traumas
- Treated with excision, steroid injections, or both
- May require tissue release for smooth contour
- Ongoing monitoring to prevent recurrence

Why Choose Dr. Jacobs as Your South Florida Gynecomastia Caretaker?
Dr. Elliot Jacobs is considered one of the foremost experts in gynecomastia surgery not just in Florida, but nationally. Patients from across the U.S. and abroad travel to his Boca Raton office for his surgical expertise and reputation.
Unlike many plastic surgeons who offer gynecomastia as one of many procedures, Dr. Jacobs has made this condition the central focus of his career. This specialization matters, especially when dealing with complex cases like severe gynecomastia or gynecomastia in overweight men. He understands the physical, emotional, and anatomical aspects of the condition and customizes each procedure accordingly.
- Meticulous technique, natural-looking results, and minimal scarring
- Board-certified plastic surgeon
- Treated over 5,000 men and adolescents
- 35+ years of experience
Dr. Jacobs’ Credentials:
- Diplomat and multi-decade member of the American Society of Plastic Surgeons.
- Pioneer of liposuction and gynecomastia surgery in the U.S.
- Designed and patented special instruments for better gynecomastia results.
- Specializes in the male physique and offers complimentary procedures.
- Welcomes patients from all identities and all locations, domestic and abroad.
- Gentle, understanding, kind, and always patient-focused demeanor.
- Castle Connely Top Doctor in South Florida, multiple years.
The Gynecomastia Surgical Process: A Step-by-Step Breakdown
A big reason guys get nervous before gynecomastia surgery is they don’t know exactly what to expect. Keeping in mind that every patient is different and no two procedures are truly alike, we find it helpful and reassuring to detail what a typical gynecomastia experience is like from start to finish with our Boca Raton-based care team.
Your Consultation With Dr. Jacobs
To help you make decisions, the first step in the gynecomastia surgical process is a personal, private consultation. Dr. Jacobs will share insights gained from more than 35 years of focus on male breast reduction. He’ll examine you, talk you through his strategy for your individual case, go over your health history, and give you a sense of the results you can anticipate. Then, the decisions are yours.
Read Our Boca Raton Gynecomastia Patient Testimonials
Our patients often say they wish they’d done this sooner. Read their personal stories to learn how male breast reduction surgery with Dr. Jacobs helped them reclaim their confidence, comfort, and freedom.
Hear Real Patient StoriesPreparing for Gynecomastia Surgery
Before your procedure, you’ll need a full medical evaluation and possibly lab work to ensure you’re a safe candidate for anesthesia. Dr. Jacobs may advise you to stop smoking and avoid anti-inflammatory medications or supplements that increase bleeding risk. Patients are encouraged to maintain a stable weight, eat a protein-rich diet, and stay physically active. Good skin quality and chest muscle tone can also contribute to optimal results and smoother healing.
The Gynecomastia Surgery in Boca Raton
On the day of your surgery, you’ll arrive at our Boca Raton office at 7:15 AM, where the team will welcome you and take your vital signs. After meeting with our anesthesiologist to review your medical history, you’ll be relaxed with twilight sedation.
Dr. Jacobs will then review the procedure, take before photos, and mark your skin. At 8:00 AM, the surgery begins with a small incision under the armpit, followed by liposuction and, if necessary, additional gland removal through an incision at the areola. By 9:00-9:30 AM, you’ll wake up feeling great, with a compression garment in place.
You’ll spend an hour or two with us, relaxing and chatting as we make sure you are fully awake and feeling great, with any discomfort well controlled. At this point, most guys feel elated! Surgery is behind them and many say it went more smoothly than they ever imagined. Most of our gynecomastia South Florida patients say they can’t wait to recover experience their new chest.
Follow-up Appointment
Within the first 24 hours post-surgery, Dr. Jacobs will call to make sure that your initial stages of recovery are going smoothly. Within 4-5 days of surgery, you will be required to return for a check-up and recovery review to make sure that you are healing correctly and you are comfortable with the post-surgery plan.
Social Readiness
Most men are surprised by how quickly they feel physically better, but emotionally, this surgery can take time to fully integrate and feel like your new normal. You may feel euphoric or even unexpectedly emotional in the first week. Both are perfectly expected. You’ll likely wear a chest compression garment for 2-3 weeks, and most return to office work in a few days, with exercise resuming in about three weeks. Socially, you might feel more comfortable shirtless or in fitted clothes within a month.
Dr. Jacobs will help guide not only your physical recovery, but your mental and emotional readiness to return to life feeling like yourself, only better.
Candidates for Florida Gynecomastia Surgery
Many types of patients at nearly all stages of life can be candidates for male breast reduction surgery:
- Men in good health with sensible expectations.
- Teens whose case has been stable for two years.
- Older men who may want to combine treatments.
- Guys who are ready to follow Dr. Jacobs’ guidance and complete care plan.
- Men whose gynecomastia hasn’t resolved with weight loss or medication changes.
- Bodybuilders or fitness enthusiasts with hormonally induced glandular tissue.
- Patients who feel socially limited or emotionally affected by their chest appearance.

After nearly 15 years of dedication to the gym and working on my physique, I decided to take the next step and address my gynecomastia. I did extensive research, consulted bodybuilding forums, and sought out professionals who understand the importance of aesthetics—every path led me to Dr. Elliot Jacobs.
From the very first consultation, it was clear I was in the hands of a true master of his craft. His transparency and honesty stood out—he’s seen it all throughout his extensive career and doesn’t promise unrealistic outcomes. Instead, he sets realistic expectations, delivers exceptional results, and has an unmatched eye for detail.
Now, three months post-op, I can confidently say that my results are phenomenal. My chest is sculpted, natural, and much rounder without any extra tissue. I honestly did not know it would make this much of a difference. The transformation has exceeded my expectations in every way. Dr. Jacobs’ precision and expertise in handling gynecomastia is second to none.
What to Expect from Gynecomastia Recovery in Boca Raton

Recovery after male breast reduction is often easier than patients expect. Most characterize the discomfort as a bruised feeling or a burning sensation in the chest that lasts for two to three days. You’ll be prescribed pain medication in case you want to take it for a short time; some guys get by with just Tylenol. Dr. Jacobs’ patients are usually ready to return to office work within three days to a week.
You’ll wear a compression garment to speed healing for about 3-4 weeks. At that point, you should be able to resume more strenuous exercise. You should feel good about your results in several days to a few weeks, but know that all traces of swelling may take three to six months to disappear.
Read John’s real patient gynecomastia story to hear one guy’s experience firsthand.
Benefits of Male Breast Reduction in South Florida
- Improved confidence and self-esteem.
- A more masculine physique.
- Better posture and reduced back problems.
- Easier maintenance of a healthy body weight.
- Long-lasting results.
- Greater ease in buying and wearing fitted clothes.
- Freedom to go shirtless without feeling self-conscious.
- Renewed interest in fitness, social life, dating, and work.
- Resolution of chafing, rashes, or discomfort from excess breast tissue.
Risks of Gynecomastia Surgery
Major risks of male breast reduction are the same as for any surgical procedure:
- Infection
- Fluid collection: hematoma or seroma
- Persistent pain
- Poor wound healing
- Allergic reaction to materials such as sutures
The operation does not endanger any major blood vessels or nerves, does not penetrate the abdominal cavity, and doesn’t disturb chest muscles, therefore major complications are extremely rare.
Risks specific to male gynecomastia surgery are uncommon when patients choose a board-certified plastic surgeon with significant experience. Some are:
- Unfavorable scarring
- Breast asymmetry
- Irregular contours
- Changes in sensation
Dr. Jacobs’ is careful to discuss all risks with prospective patients, and he performs a thorough analysis of each individual’s health and lifestyle as well. You will not elect to have gynecomastia surgery without this important step.
See What’s Possible: Before & After Male Breast Reduction in Boca Raton
Browse real patient results in our Gynecomastia Before & After Gallery to see what male breast reduction in Boca Raton can do for you. Every result reflects Dr. Jacobs’ surgical skill – plus the personal freedom that comes with looking how you’ve always wanted to feel inside.




Enhance Your Gynecomastia Surgery with Other Male Cosmetic Procedures
Many men choose to address multiple physical, confidence-lowering concerns in one complete transformation. Dr. Jacobs specializes in procedures that help you feel more in control of your body, image, and life. Together, you can create a custom surgical plan that aligns with your lifestyle and goals – plus helps trim down total surgical time and costs.
Abdominal Liposuction & Mid-Body Contouring
Stubborn fat in the abdomen is a common concern even for guys who work out regularly. Liposuction can re-define the waistline, reduce that stubborn belly fat’s appearance, and enhance the results of gynecomastia surgery for a more athletic upper body.
Neck Lift
A sharp jawline adds definition and masculinity to the face. A neck lift helps remove excess fat and sagging skin under the chin and along the jaw, making a dramatic difference in profile and overall appearance – especially when paired with chest contouring.
Torsoplasty
A complete upper body transformation that brings reshaping and retoning to not just the chest, but the abs and hip rolls. Creates a rectangular and traditionally more masculine frame that still looks and feels proportionate for you.
Book a Gynecomastia Consultation in Boca Raton
You don’t have to live with the burden of your less-than-ideal chest. Dr. Jacobs offers real, life-changing solutions, personalized support, and international expertise, all to help you move forward with your life, looking and feeling great.
Contact UsContact Us
Reach out to Dr. Jacobs today to schedule your consultation!
Gynecomastia Surgery Boca Raton FAQs

How Does Dr. Jacobs’ Gynecomastia Approach Differ?
During Boca Raton male breast reduction surgery the goal is to produce a trim, taut, and contoured chest that blends in with the surrounding areas of the body. Men do not want to have surgery to remove their gynecomastia but replace it with lots of scars – that is trading one problem for another.
There is also an art to doing this surgery – knowing how much tissue to remove and how tissue much to retain. When a guy is on the heavier side, removing too much tissue can result in contour irregularities and discord between the chest and the surrounding areas. In these cases, the surgeon must leave some extra tissue for a normal appearance.
The surgeon should also examine the entire chest, not just the breasts. It is possible for fat to extend into the armpits or lateral chest. For a truly contoured chest, these areas should also be treated and contoured at the time of the initial surgery. Otherwise, the patient would have a flat chest and residual fat bulging on the sides of the chest. Some men may suffer from excessive sweating of the armpit area. This, too, can be addressed at the same time.
Is Gynecomastia Life-Threatening?
Gynecomastia can be small – just an accumulation of excess breast tissue beneath the areola, which results in elevation of the areola alone. Or, it can be very large, assuming the appearance of a large, pendulous female breast. Or anything in-between. Since it is a non-life-threatening condition, the decision to seek a surgical remedy is entirely individual. Some men accept it and go on with their lives. For others, it can become a significant negative focus in their lives and they will only find solace by having surgery.
How Does Gynecomastia Develop?
Gynecomastia can be defined as excess tissue on a male chest. That tissue is either fat or breast tissue (gland) and most often a combination of both. All men have a certain amount of breast tissue on their chest, usually directly under the areola – that is normal. Gynecomastia develops when that breast tissue begins to increase or there is additional fatty tissue. There is no such thing as pseudo-gynecomastia, which purports that all the accumulation on the chest is simply fat. That is not true. There is always some amount of breast tissue present as well.
When present in our Florida patients, gynecomastia consists of breast tissue that is concentrated directly under the nipple/areola. It then spreads out in a horizontally-oriented, oval distribution over the lower portion of the chest. As it spreads out, it begins to join and blend in with fat tissue, in a manner similar to fingers interlocking with one another. There is no wall or capsule which separates the breast tissue from other tissues – they simply grow together. Therefore, there is no way that a surgeon can remove only the breast tissue and leave the remaining fat intact – or vice versa.
Should I Lose Weight Before Gynecomastia Surgery?
Many men wonder if losing weight before gynecomastia surgery is recommended, and the answer is yes. Formerly overweight patients generally fall into two categories:
1. Those whose skin can bounce back after surgery. Men who have lost a moderate amount of weight and have good skin quality often experience skin tightening during the healing process. Dr. Jacobs uses a combination of gland removal and liposuction with specialized instruments, leaving minimal scars for a masculine chest.
2. Those with loose skin that may not tighten. For these patients, Dr. Jacobs may recommend skin removal and nipple repositioning to achieve a more sculpted chest, though this comes with the tradeoff of larger scars.
Does Skin Quality And Elasticity Impact Gynecomastia Results?
Skin quality and elasticity play a significant role in breast reduction. When skin is stretched, such as from weight gain, the elastic fibers lose their ability to bounce back, leading to permanent loss of elasticity. This is similar to how a stretched rubber band remains loose, and it can result in issues like stretch marks, which cannot be repaired. Factors like smoking, sun exposure, and aging also contribute to diminished elasticity. For overweight men seeking male breast reduction, the decision on the procedure depends on skin quality. A trade-off must be made between minimal scars with a less-than-perfect result or a more contoured chest with additional scarring.
